School has officially begun for the year and with that comes an increase in activity levels for many children. As the fall and winter season approaches, many kids will participate in school sports as well as extra-curricular organized sports and activities. This ramp-up in exercise levels can sometimes lead to aches and pains, particularly in young children who are still growing at fast rates.
The term “growing pains” refers to this sort of injury. This pain is muscular in nature and occurs because bones are growing and changing at a faster rate than the muscles can keep up, which puts added stress and tension on the muscles. This can be more prevalent in children who participate in sports all year long, or children who play multiple sports at the same time.
Common Growing Pains
Sever’s Disease: pain in the back of the heel where the Achilles tendon attaches.
Shin Splints: pain in and around the shins.
Osgood Schlatter’s Disease: pain below the knee from the quadriceps muscle pulling on the shin bone.
Symptoms of Growing Pains
Pain in the thighs, knees, shins, or ankles.
Pain after playing sports or engaging in activity.
Pain at night when sleeping.
Pain is described as an “ache” or “burning.”
Physiotherapy and Growing Pains
Physiotherapist Nada demonstrating stretches that can be relieving for Severs Disease
Physiotherapy treatment is a very effective way to treat and manage activity-related pains in growing children. The aim is to reduce inflammation and improve muscle flexibility and strength. This includes techniques like mobilizations, manual stretching, and soft tissue work. The physiotherapist can also instruct you on how to manage your symptoms at home and what exercises to do to effectively target the area.
Single leg step ups for Osgood Schlatter DiseaseSingle leg heel rises used for Severs DiseaseExercises that are beneficial in strengthening relevant muscles in individuals with Severs or Osgood Schlatter Disease
If your child is experiencing pain and discomfort with exercise, book an initial assessment here with one of our physiotherapists. They will design a treatment program individually tailored to your child’s needs, age, and activity level.
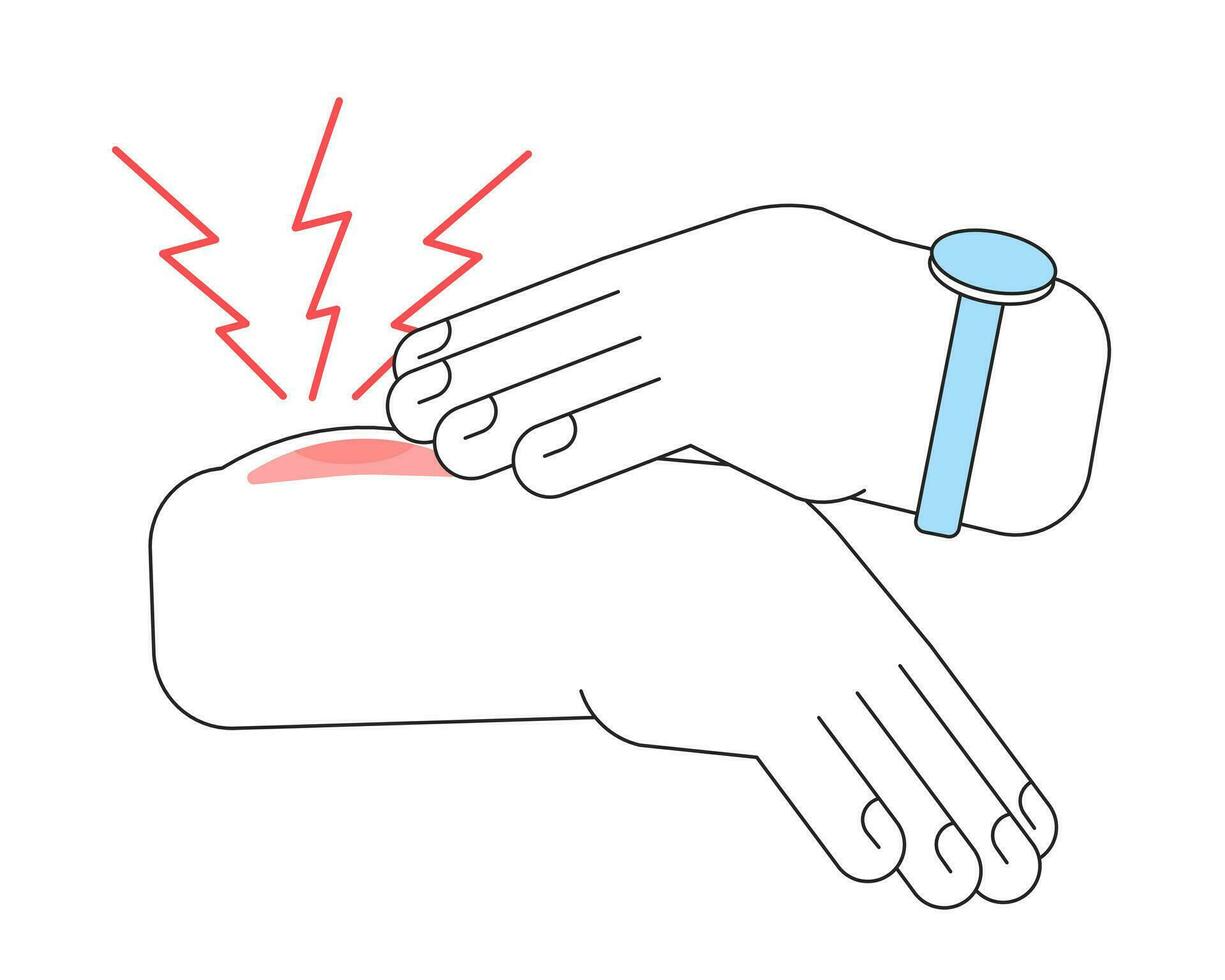
Are you familiar with the term contusion? A contusion is the medical term for a bruise. Muscle contusions are a result of direct impact or trauma to the area. The most common sites for this to occur are the thighs, knees, arms, or calves. This direct impact leads to muscle bleeding and fiber damage which is what causes the swollen and reddish-purple bruise appearance. Contusions can occur from any form of contact sport, rough play, falls, or accidents where the body bangs into a hard object. Muscle contusions are different from muscle strains, which usually occur from sudden fast movements or overworking a muscle more than it’s used to.
Contusions are graded by their severity as Grade 1, 2 or 3.
Grade 1 contusions produce minimal pain and swelling. You may feel some soreness and stiffness with movement, but your range of motion is likely unaffected.
Grade 2 contusions will likely have more consistent pain and swelling may be present. You may not be able to walk or move normally without experiencing pain. Your range of motion may be decreased.
Grade 3 contusions are the most severe. Pain with any small movement will be present and significant swelling will occur. You may need to use crutches to help you walk. Strength and range of motion are significantly impacted.
Physiotherapist Kristina working on range of motion after an arm contusion
After a contusion, a physiotherapist can provide you with education on how to properly care for your injury and promote healing at home. Physiotherapy can also help restore your range of motion and strength to the affected area through movement and exercises. For more severe contusions, manual therapy can gently mobilize the muscle and surrounding tissue to promote blood flow and good alignment of the healing muscle fibers.
If you have experienced a muscle contusion, schedule an assessment here and one of our physiotherapists will be happy to assist you.
Acupuncture is becoming increasingly popular, yet many people remain reluctant to use it as a form of treatment. So, what exactly is it, and how can it help you? We answer these and more below!
What Is Acupuncture?
Acupuncture is a therapeutic technique of inserting fine, one-time-use pre-sterilized needles into very specific points along the body to assist in pain management and healing of injuries. Patients often ask us if acupuncture is painful. The needles used for acupuncture therapy are extremely fine – patients likely feel a small poke but once the needle is inserted, most patients do not feel much pain.
How Does It Work? – Traditional Chinese Medicine
Acupuncture was developed more than 3,000 years ago in China. In Traditional Chinese Medicine (TCM), injuries or illnesses are believed to be the results of an imbalance of energy within the body, specifically within meridians, which are channels of energy flow throughout the body. Acupuncture is used to help restore energy balance by placing fine needles at specific points along these meridians.
How Does It Work? – The Gate Control Theory of Pain
Although acupuncture is an ancient practice in Eastern medicine, its use in Western medicine is relatively recent. Though the exact reason why it works is not totally clear, Western medicine has several different theories as to how acupuncture helps with injury recovery. One of those is the Gate Control Theory of Pain.
The Gate Control Theory of Pain outlines how pain signals reach the brain from the spinal cord. In simple terms, if the ‘gate’ is open at the level of the spinal cord, a pain signal can pass through, reaching the brain where the pain is perceived. If the ‘gate’ is closed, a pain signal cannot pass through, and therefore the brain does not perceive pain. So, using this theory, applying a non-painful stimulus when someone experiences a painful stimulus can activate the closing of the gate and decrease the pain signal to the brain. An example of this would be if someone bangs their knee against a hard surface. Usually, our first instinct is to rub the knee (a non-painful stimulus), which helps us feel less pain.
What Injuries Can Be Treated With Acupuncture
Acupuncture can help in the healing process of many muscle and joint injuries. However, it is important to note that it won’t exactly heal these injuries. For example, if a muscle is torn, acupuncture will not repair the tear. However, it can assist in the symptoms associated with the tear, primarily by decreasing pain. Acupuncture has been used to aid in the recovery of a number of injuries, such as rotator cuff tendonitis, tennis elbow, and mechanical neck and back pain.
What Are The Risks Associated With Acupuncture?
The risks associated with acupuncture treatment are relatively minimal. The most common side effect is soreness and/or bruising in the region where the needles are inserted. The risk of infection is extremely LOW since the needles are pre-sterilized and used once. Some people might feel light-headed or dizzy after acupuncture treatment, so it is important to make sure you are well-hydrated and have eaten before your treatment session. If you are pregnant or have had other medical conditions (ex., cancer, stroke, etc.), there are certain points or areas that your practitioner will avoid. This is why it is extremely important to be thorough when reporting your medical history to your practitioner.
If you would like to learn more, ask your practitioner to discuss whether it would be an appropriate option for you, or book an initial assessment with us here!
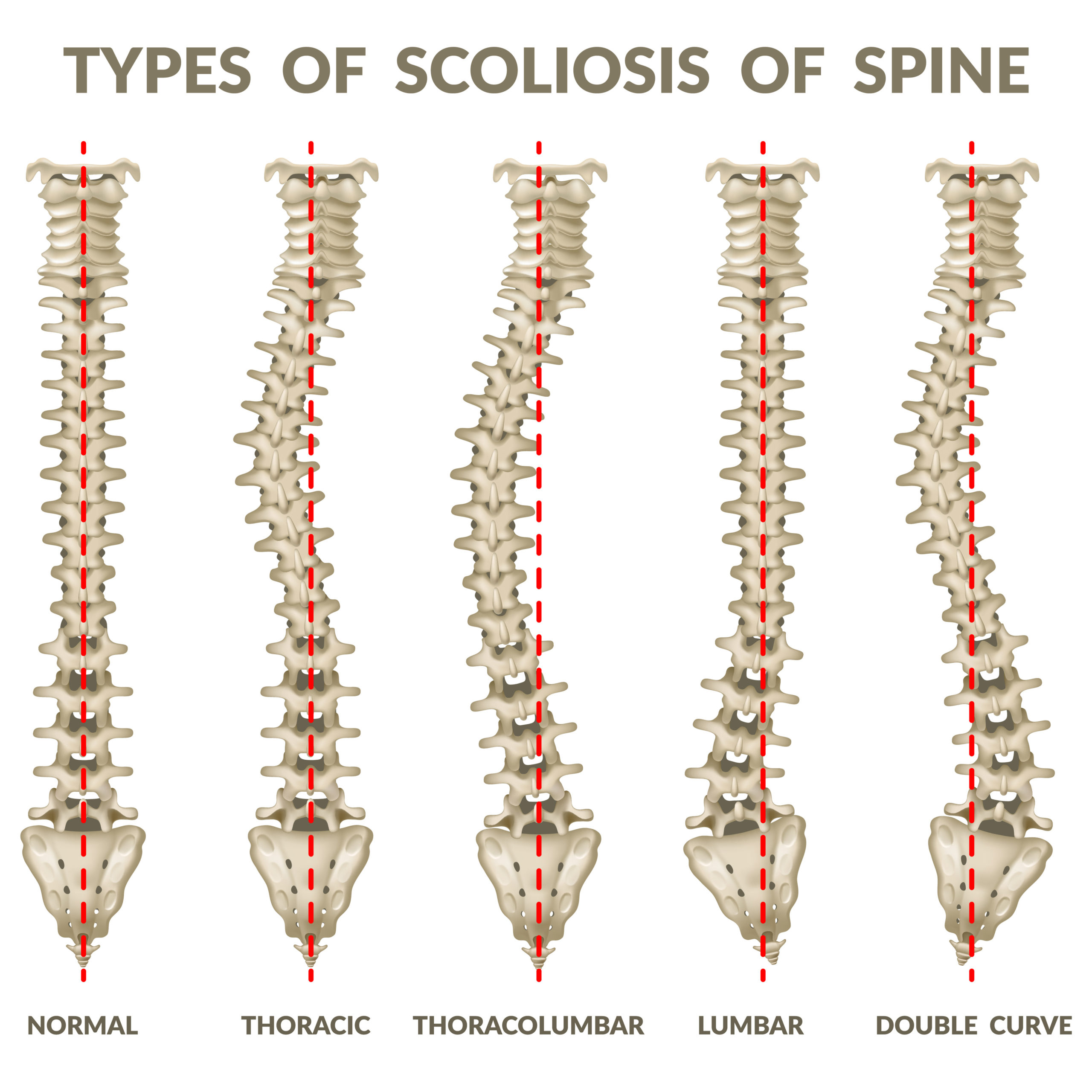
A normal spine has three main curves: cervical lordosis, thoracic kyphosis, and lumbar lordosis. These curves occur in the frontal plane, meaning they curve front to back. A scoliotic curve curves to the side.
Therefore, a scoliosis refers to when the vertebrae in the spine do not follow a straight line but are curved sideways. Sometimes they can also rotate, or twist, like a corkscrew.
A small scoliotic curve may be barely noticeable by eye, or it might be so slight that an X-ray (or MRI) would be needed to measure it. In those cases, the scoliosis is unlikely to cause any issues.
However, when a scoliosis is present in children, the curve may continue to grow until their skeleton is fully developed. This means that if the curvature becomes significantly large, it can cause more than just bad posture.
It can lead to headaches and back pain, loss of normal range of motion, digestive issues, affect breathing, and eventually cause early arthritis due to the unusual pressure on some of the joints, etc.
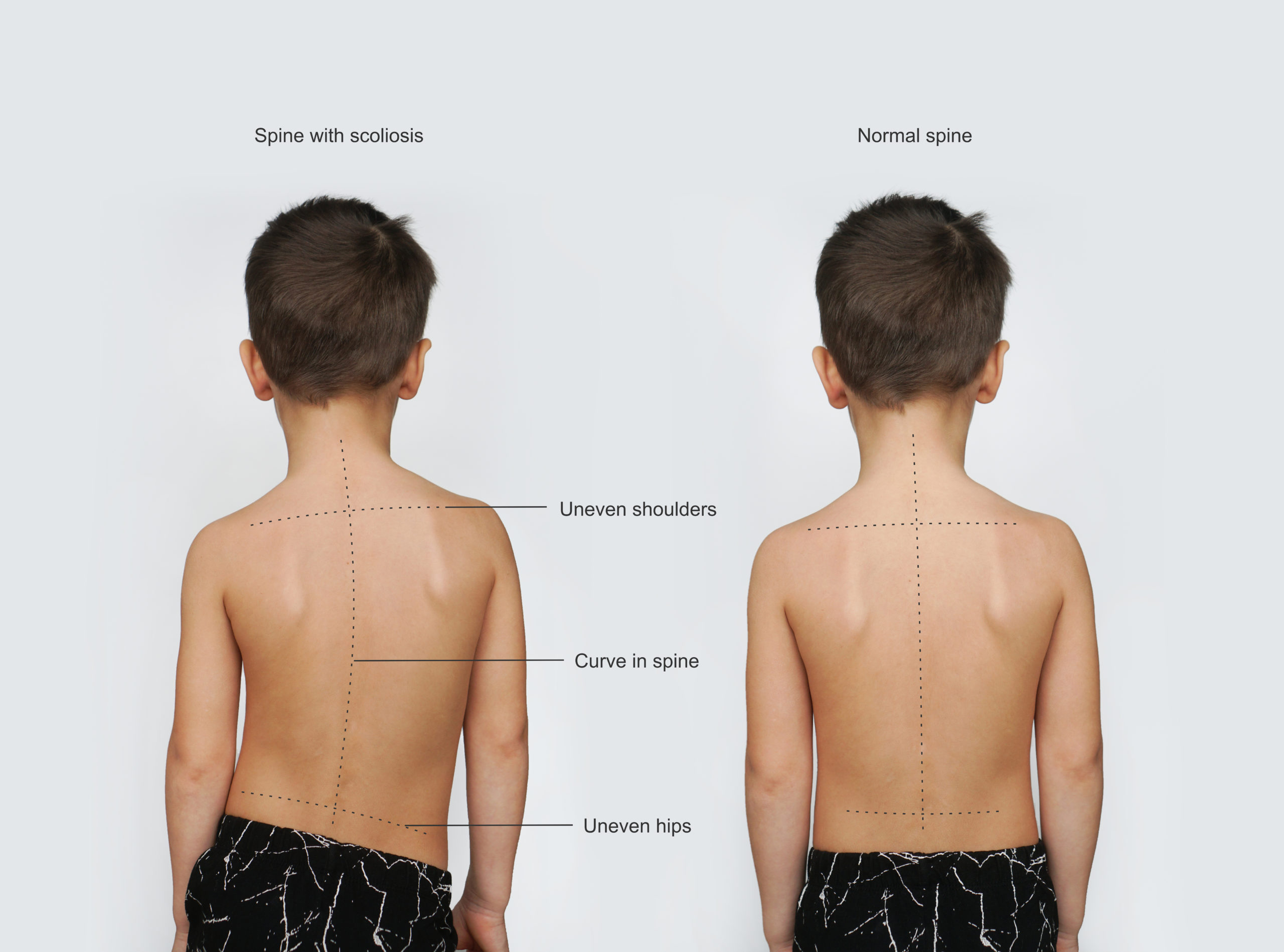
Observable symptoms of Scoliosis
The head is not centered with the rest of the body
Uneven shoulders
Constant leaning to one side
Difference in hip height
Difference in shoulder blade height or position
Uneven arm position as the arms hang on both sides of the body when the child is upright
A sideways curvature of the spine when the child bends forward
Signs Of Scoliosis. Normal healthy spine and curved spine with scoliosis.Scoliosis in children
Causes of Scoliosis
Most commonly (80-85% of the time), scoliosis is idiopathic, meaning the cause of it is unknown. In some cases, the development of idiopathic scoliosis can be due to a genetic predisposition.
While it can be diagnosed at any age, it is usually diagnosed in kids 10 and older.
There may be a correlation with poor posture as well. This is where we can differentiate if a scoliosis is functional or structural.
A functional scoliosis develops due to certain postures and compensations that are likely due to muscle tightness and imbalance. In those cases, the spine appears to be curved but is not actually.
A structural scoliosis originates in the spine and cannot be corrected by correcting posture and muscle imbalance
Less commonly, scoliosis can be:
congenital, meaning that there were problems in the spine before a baby is even born. Usually, the spinal bones are either not fully formed or are fused in ways they should not be.
neuromuscular, meaning that conditions that affect the nerves and/or muscles of the body (such as cerebral palsy or muscular dystrophy), will affect their ability to support the spine, leading to the development of a scoliotic curve
Severity of Scoliosis
Mild – Curve is less than 25 degrees, and risk of progression is 22%
Moderate – Curve is between 26-40 degrees, and risk of progression increases to 68%
Severe – Curve is above 40 degrees, and risk of progression is quite high at 90%
What to do about scoliosis?
In mild cases, if there are no symptoms or cosmetic concerns, then often the course of action is nothing.
However, until the child or adolescent is fully grown, the risk of progression is there. This means that the scoliosis should be monitored regularly (usually annually) and a referral to physiotherapy might be appropriate for preventative strategies and education.
In moderate cases symptoms are more likely, such as headaches, back pain, digestive issues, and fatigue with activity. A brace is often recommended to reduce the risk of progression and give the organs more room.
Physiotherapy and sometimes other disciplines, such as registered massage therapy and chiropractic, may also be an effective adjunct to bracing to help with symptoms and postural correction / education.
In severe cases, especially if a curve is above 50 degrees, a brace is not going to be able to able to slow progression, and surgery is likely to be recommended. Surgery usually involves spinal fusion to realign the vertebrae.
There have been many advances in surgical correction of scoliosis so the kind of surgery required will depend on the type of misalignment, the severity of symptoms, and the location of the scoliosis.
Overall, surgery has good outcomes.
What can Physiotherapy do about my child’s scoliosis?
In mild cases, treatment is preventative:
Postural correction and education
Postural exercises to correct muscle imbalances that have developed due to the scoliosis
Manual therapy (soft tissue release, joint mobilizations) to help improve flexibility and restore range of motion that have been impacted by the scoliosis
Postural taping to give proprioceptive feedback to the body and provide awareness to the child so they can better self-correct as they become aware of how their body is sitting in space
In moderate cases, treatment also helps to eventually wean off bracing while managing any associated symptoms.
In severe cases, physiotherapy might be helpful post-operatively to correct the muscle imbalances that had developed pre-operatively.
Yes, exercise and sporting activities (especially ones that focus on core strength) are encouraged!
In the severe cases, there may be some sport restrictions following a surgery. This is usually because after a fusion there will be some permanent loss of overall range of motion. However, kids often are able to return to sporting activities within 6 to 9 months after surgery.
Infants (0-12 months) have many important milestones to hit during their development. Sometimes it seems like every week they’re learning something new!
Their brains and bodies are integrating so much information about their environment and how to interact with it. This includes sensory information (sight, smell, sound, touch).
There are different kinds of milestones:
social and emotional skills,
language and communication skills,
feeding,
sleeping,
sensory such as hearing and vision,
gross motor and fine motor skills…
Today we will focus on the importance of gross motor skills, specifically in regards to tummy time!
What is Tummy Time?
Tummy time is when infants spend a certain amount of time, playing (or at least staying) on their tummy.
It is important to note that during various stages of development the term “tummy time” can be a lot broader. It does not exclusively mean placing babies on their stomachs. It can be modified so that they are on their knees and leaning on to / playing on an inclined surface or toy. But for the most part today we will talk about being on their tummies!
Modified plank onto a bolster is great for developing arm strength and still counts as tummy time!
Why is this important?
Time babies spend playing on their tummy can hugely impact their gross motor development. It is basically a workout!
As they learn to push up through their hands, they develop upper body strength.
As they learn to move their neck against gravity, they develop neck strength and control.
As they eventually learn to get onto their hands and knees (and crawl), they develop core and hip strength.
By spending less time on their back, this improves neck tightness issues such as torticollis, and any skull deformities such as Plagiocephaly (Flat Head Syndrome) which develop as a result of the one-side head turning preference typical of torticollis.
Tummy time is also a gateway totransitional movements.
Initially, babies begin to learn rolling over from back to tummy and back again. Being on their tummies is more interactive than being on their stomachs, and they get a better view of their surroundings.
But rolling over is not a very efficient way of getting around. By pulling up through their arms (the army crawl), they can get further in a straight line. By getting onto hands and knees to crawl, they can do this much more quickly and efficiently.
Building up the strength in their core, neck, arms, and hips lays the foundation to learn to transition from four-point position (hands and knees) –> pulling up to kneel –> pulling up to stand –> cruising –> walking.
Modifying tummy time to high kneeling and leaning forward to play with a toy… the important thing is still weight-bearing through arms and legs!
Transitioning from hands and knees to hands and feet (“bear” or plantigrade position) is how they eventually learn to stand up on their own.
Ideally, they are learning all of these new transitions and movement patterns symmetrically on both sides. Hand and side dominance will begin to show at its earliest around 18 months (but is more solidified between 2-4 years of age), which means that during their development, infants should learn and demonstrate all movement patterns symmetrically.
Think about what tummy time entails… pushing up through the hands, army crawling, and eventually hands and knees crawling. Infants are using their whole bodies and in order to move around to reach an object of interest, they are learning symmetrical and reciprocal movement on both sides of their body to achieve this goal. The reciprocal motion of crawling later becomes a natural reciprocal motion when walking: opposite arms and leg motion!
This symmetry also means that infants are not developing tightness/weakness more on one side than the other, leading to muscle imbalances.
In other words, if your little one is not spending a lot of time on their tummy, you can expect their motor milestones to be more delayed.
When can you start Tummy Time?
You can start super early! According to the American Academy of Pediatrics, you can even do it the first day home from the hospital! (Of course, making sure to support their head as you change their position.)
How often should infants spend in Tummy Time?
Initially, you’ll be doing very short bouts. Even 3-5 minutes, 2-3x day is okay. Gradually, as your baby gets stronger and more comfortable, you can increase the time duration and frequency throughout the day.
How to do Tummy Time?
In the beginning, when your baby is still newborn (0-2 months) and does not have the strength to lift up much against gravity, you will be providing them with support.
This could be resting on your chest (skin-on-skin is a great way to bond!). This way they are inclined rather than fully horizontal which is harder, and you are able to assist them with your hands.
It could be on their playmat but bolstered at the chest with a rolled towel, small pillow, or Boppy Pillow so they are still inclined and have the support under their chest that their arms cannot yet fully provide.
Gradually, as you notice they are starting to rest more effectively onto their forearms and are lifting up their heads higher and for longer periods of time, you may sometimes skip using the pillow support and increase the time spent on their tummy.
If colic, or other issues, are limiting your baby’s ability to practice tummy time, speak to your physician and/or local physiotherapistfor alternative strategies!
Get creative with tummy time 😉
Where to do Tummy Time?
Everywhere! Exposure to different textures, surfaces, and environments is great practice.
You may notice that even their clothing makes a difference. Some infants do not tolerate being bareskin while others may dislike tummy time in their clothes. This can be a sensory issue, or perhaps the clothing (or carpet / duvet, wherever they are practicing) may be cumbersome and making it hard to move around.
Different places to try:
Chest on chest
Lay baby across your legs, raising one knee higher to raise their chest
Tummy-down carry
Floor
Bed
Is it ALL about Tummy Time?
Of course not!
While it is important that babies spend time on their tummies, having an equal opportunity to practice sidelying, sitting, side sitting, high kneeling, etc. (as appropriate for their age) is also important. Otherwise, they will get overly strong with one set of muscles and not develop others.
Lastly, the most important thing of all is giving them the opportunity to learn on their own! If you are always picking them up place them somewhere, or handing them their toys instead of having them try to get there on their own, then they won’t have the opportunity to problem solve and get stronger. 😊
A lot of people’s response is putting the hands on the waist at the top of the pelvic bones. The true hip joint from a Physio’s perspective is basically where the legs attach into the torso. The crease of the groin delineates this. You can also landmark by placing the heels of the hands at the top of the pelvis and the finger tips reach the greater trochanter of the long bone of the femur.
The hip, like the shoulder is a ball in socket joint. The joint is made of the hip socket, or the acetabulum of the pelvis), and the ball-like top of the thigh bone (the femoral head). The shoulder is more mobile and the hip joint is more stable. It is surrounded a cartilaginous labrum, strong ligaments connecting bone to bone, and big strong muscles.
What is developmental dysplasia of the hip (DDH)?
Hip dysplasia in babies occurs when the socket, or acetabulum is too shallow to cover the head of the femur / thighbone. The issue can also be with the femoral head. Dysplasia of the hip can range in severity and can affect one or both hip joints. Babies with dysplasia may have minor looseness of the hip to joints that come easily out of the socket.
It is common during well baby checks for babies to have their hips checked. This means that most babies are diagnosed with hip dysplasia in the first few months. This also means that treatment or monitoring can begin early.
If there are concerns of hip dysplasia in infants it is usually diagnosed with an X-ray or ultrasound imaging.
Common Symptoms of Developmental Hip Dysplasia:
One leg may appear to be shorter (this is the affected side)
The folds of the skin at the buttocks or thighs may look uneven from right to left
With movement of the hip there may be a sensation of popping
Less mobility or movement on one side
Limping once a child is walking
Toe walking
Waddling or duck-like gait.
As a parent or caregiver if you notice these and the baby has not been identified as having hip dysplasia, bring it to the attention of your paediatrician or family doctor for monitoring. It is important to identify and treat hip dysplasia early for best outcomes.
Causes of Hip Dysplasia?
It is not always know what the case of hip dysplasia is in infants. It is believed that there are many factors that can lead its development.
The shape of the pelvis may have a genetic component. If there is a family history of hip dysplasia, such as a biological parent or close relative.
Girls are more likely to have hip dysplasia
Left hip. The left hip is more commonly affected than the right.
Birth order – babies who are born first are more likely than later Bronte babies to have hip dysplasia. This is because the uterus is a tighter fit.
Birth weight over 9lbs
Decreased amniotic fluid volumes
Twins. Infant twins are more likely to have hip dysaplsia for the same reasons as above.
Feet down or breech positioning during pregnancy. The legs may stay extended rather than tucked up in the fetal position. Staying in a straight position may inhibit the hip joints from developing properly.
Swaddling the infant tightly with the legs extended. This may inhibit the healthy / natural joint development .
Non-Surgical Treatments for Hip Dysplasia:
Observation / Wait and See
If the baby is less than 3 months of age and the hip joint is stable a wait and see approach is often taken. Education regarding swaddling, positioning and gross motor skills are helpful here. This may be done through the paediatrician or specialist as well as a Physiotherapist who works with babies. It is possible for the hip joint to form well on its own as the baby grows and develops.
Harness or Brace:
If the hip joint is unstable or more shallow it may be recommended that they wear a harness or brace. A harness called the Pavlik harness is used for babies under 4 months. It holds the hips in place and allows the legs some movement. It is generally worn 24 hours a day over 8 to 12 weeks. They will be monitored using ultrasound over this time. after the use of the harness they will be monitored over the next few years depending on the severity of the original dysplasia.
What is the Role of a Physiotherapist in Treating Hip Dysplasia in infants?
Physio for hip dysplasia depends on the age of the patient. It also depends on the chosen course of treatment.
Physio can be used to strengthening the muscles around the hips and work on gross motor skills. Gross motor skills include things like rolling, meeting feet to hands, crawling, and sitting. This is important if the baby is also slightly delayed by use of the brace or harness.
If the baby is not braced or harness, the Physio will comment on ideal hip positioning. Avoiding straight legs with knees together and encouraging the hips to fall apart to the sides. This is called a jockey position, or frog position. Using a baby sleep sack is another way to help this natural positioning.
Your Physiotherapist can help identify the positioning that looks best for your little one as well as baby wearing positions or carrying positions. They will also discuss how to optimally swaddle to avoid the tight legs extended position for your baby.
Some of our North Oakville Physiotherapists have a special interest in helping your little ones along. We do see and treat infants and children in our North Oakville Physio and Massage clinic. We are also able to provide follow-up Physio treatments and consultations via video. Private Physiotherapy for infants and children can be covered by your extended health plans. We are able to direct bill to most insurance companies.
Contact us to book in with one of our Halton Physiotherapists who treats infants and children also.
When our Oakville Physiotherapists are giving a home program for little ones, they often don’t follow the same “rep / set” scheme as teens and adults. They often resemble more play based activities!
These exercises for our young patients are given for different reasons and have bonus outcomes!
We love giving different animal walking exercises!
Benefits of Animal Walking:
Bilateral coordination – using both sides in a coordinated way.
Upper body strengthening
Lower body strengthening
Core strengthening
Vestibular input (input into the brain, inner ear and eye systems)
Positive carry over into other areas of your child’s activities.
They’re fun!
A Physiotherapist that works with kids may have a specific purpose for giving a specific animal walking exercise, but all of them are fun to try!
Examples of Animal Walking:
Bear crawls
Crab walks
Frog jumps
Bunny hops
Cat crawls
Snake slither
Duck waddles
Donkey kicks
Elephant swings
Flamingo hops
Horse galloping
Inchworms
If your little one has a lot of trouble with one, not to worry, keep trying and focus on some easier ones to start. These are great for indoor activities in poor weather and on short breaks with virtual learning.
Keep it interesting by having them choose a card with an animal walk, make small scavenger hunt using different movements to go from station to station etc!
Our North Oakville Physiotherapists see kids both in clinic and virtually for physio assessment and treatment. Some things we treat are: development coordination disorder, delayed gross motor skills, hypotonia, toe walking, recovery after broken bones and being immobilized in a cast.
More parents in Oakville and Halton have been opting for their elementary age child(ren) to participate in online learning. Most high-school students in Halton and Ontario are in a hybrid model with a combination of online and in-person learning.
We have seen so many adults in our North Oakville clinic, struggling with their home workstations. These workstations, chairs and desks have not been designed full days of work. People have been complaining to our Oakville Physiotherapists, and RMTs of tension headaches, low back pain, neck pain and shoulder pain, all from sitting and working in less than ideal positions.
This discomfort of the body is distracting when you’re trying to work, sleep and live.
Now imagine the same for your little ones.
Just as a Physiotherapists are able to make recommendation for the adult work ergonomic set-up, we are able to help optimize an online school area for your littles.
Getting started with an online school setup:
Do their feet touch the floor? Let’s start from the bottom up. A child’s feet should be able to touch flat on the floor. It may be necessary for the rest of the set-up to bring the floor up to the child, using a box or step.
The Chair. Your students back should be able to touch the back of the chair, while keep the feet flat. There should be space between the calves and the seat of the chair.
The Device. Most people have their kids set up on a laptop, chrome book, or I-pad of some type. While these tools are more portable (bonus!), sitting at them for long periods of time may not be ideal. There is a tendency to slouch and curl over these tools. Students may not take normal related breaths in these positions and the neck and shoulders may start bothering them. Ideally have the top of the screen close to eye level, and a keyboard on a tray so the elbows can bend at 90*
Change it up. The best position is the next position. Provide a few choices of workstations for your online learner. An area to sit and an area to stand are both great.
Variety is the spice of life. While the primary chair is best to a typical stationary chair, spending some time on a stool, an exercise ball, or with feet on a wiggle band can wake up the body and increase attention to the task.
Break Time – use the break times for actual movement and exercise. Get the heart rate up and the breathing heavy. Aerobic exercise helps a person focus on the task following, more effectively.
Fiddle. Providing doodle paper and a stress ball or putty. Keeping hands busy during lecture or video time can help with focus.
Rock a Weighted Lap Blanket. Sitting for long periods of time can be challenging for anyone. Providing some weighted support across the thighs can help relax a person and help with focus.
Many students are setup with ear phones to keep noise to a minimum, and when there are more than one student in a household. It is important to have earphone that are designed for children, where there are volume controls. Our friends at Chorus Speech and Hearing would be better able to suggest specific tools.
Do you need help setting up your child’s workstation to optimize their online learning?
Our Oakville Physiotherapists are here to help!
Contact us to arrange a virtual appointment where we can meet your child and access the space available.
We hear lots of these terms flying around when you are around kids. Milestones, motor skills, fine motor skills, gross motor skills….
What are they, and why do they matter for you and from a Physiotherapists perspective? Our Oakville Physio Kristina will delve deeper into these topics here!
What are motor skills?
Motor skills are learned movement patterns, which are the result of the brain, nervous system and muscles all working together. Most motor skills are marked by certain childhood milestones.
What are gross motor skills?
Gross motor skills are bigger movements that don’t require a lot of finesse. They are performed by bigger muscles working together, such as the muscles in the arms, legs, and trunk. Crawling, balancing, walking and jumping are examples of locomotor gross motor skills.
Catching, throwing, and kicking are examples of object-control gross motor skills.
What are fine motor skills?
Fine motor skills are smaller movements that require more precision and refinement. They are performed by smaller muscles, such as the muscles of the hands, fingers and toes, or the lips and tongue while speaking. For example, picking up small objects, using cutlery, writing, cutting with scissors, drawing or playing the piano, etc.
Interestingly, the development of fine motor skills are supported by having a strong core as well as muscles close to the torso. Having shoulders, hips, back and chest strength and endurance helps provide a stable base of support to operate your smaller muscles off of.
What are motor milestones?
Motor milestones are the major developmental tasks that are learned during a specific time of development. They are usually tracked by regular pediatrician appointments with your baby.
For example, pulling up to stand and cruising the furniture are gross motor skills usually achieved at 10-12 months. Using the thumb and index finger to pick up small objects are fine motor skills usually achieved at 10-12 months.
There are other types of milestones, such as sensory, communication, and feeding milestones.
Motor milestone logically lead into other tasks. For example tummy time and propped tummy time helps strengthen the back of the neck and shoulders. This helps progress to four point point positions. Four point positions (hands and knees) helps strengthen the muscles around the core, hips and shoulder girdle. Reaching in four point positions helps transition to crawling.
What is the role of Physiotherapy in motor skills?
Children can be delayed in the learning of certain motor skills due to a variety of reasons.
For example, developmental coordination disorder (DCD). As the preschool years (ages 3-5) are often a critical period for learning certain motor skills, if your child is having difficulties, it is best to address them early on to avoid further delays later on.
Your chips teacher may mention that they have concerns with how your child moves. You may even notice when they are playing with other children their age that they are not matching up with regards to running, jumping and ball skills.
Additionally, after injury at any age, certain motor skills may need to be relearned or refined. For example, returning to regular activity after a fracture. Restoring strength, range of motion, proprioception, speed, endurance, as well as the appropriate movement patterns is a part of that.
Physiotherapy for a child can provide specific rehabilitation exercises and strategies to help develop, relearn, or refine the lacking or delayed motor skills. If there are physical impediments that are contributing to motor skills issues, they can be addressed in physiotherapy through manual therapy, modalities, bracing, gait aids, and/or other devices.
Keep in mind that learning fine motor skills does not translate into learning gross motor skills and vice versa. Progress in one area does not guarantee progress in another. If a child or adult is struggling with a particular set of motor skills, they may need more specialized exercises and strategies to address these difficulties.
Here at Oakville’s Palermo Physiotherapy and Wellness we treat ages zero and up when it comes to motor skills!
There are a variety of factors that play a role in the development of torticollis (stiff or tilted neck) and plagiocephaly (flattened head areas) in infants. It can be related to factors in-utero (space, first baby, location) and birth related factors (assisted or complicated deliveries). One large contributing factor is also the reluctance of parents to place their babies on their fronts as well as keeping their babies in carrier (container baby). Our Oakville Physiotherapists have treated many infants and babies with torticollis with an interplay of these reasons.
The contributing factors within our control are is the resistance to tummy time and use of containers the can be switched to the car, the stroller and to swings.
We are far more educated due to SIDS campaigns about the risks of babies sleeping on their tummies. The unfortunate carry-over is the fear or resistance to placing baby on their tummy during waking hours.
Another factor may be that baby is fussy on their tummy and doesn’t tolerate much time. While this may be the case, this fussiness should be explored. How is their latch, do they have reflux? are they colicky? Perhaps with these symptoms they should also be assessed by a qualified paediatric dentist for tongue or lip tie.
When a baby is born the bones of the skull are not fused. They are flexible and the shape of the head is determined by the position the baby assumes. The first 6-8 weeks is very important in the development of the head and skull. A baby that stays on their back or in a carrier all the time is at risk of developing a flattened spot on the skull. If baby always has their head turned to one direction they could develop a flattened area on the side of the head. This can also carry over to facial asymmetries. This can be alarming for some parents cosmetically. With a flattened area, babies head is more likely to turn to that side which leads to a tightening of the neck muscles on that side. This is difficult for baby to correct as they have not developed their neck muscles against gravity.
Tips to Prevent the Development of Torticollis and Plagiocephaly:
Make sure baby has a variety of position changes when they are awake. These changes in positions are also important for the baby to strengthen muscles used for the development of gross motor skills such as rolling, crawling, and sitting.
Tummy time and sidelying time that is supervised is important. Newborns can be places in chest to chest or an inclined position during snuggle times. As baby gets older adjust where the toys are so baby looks both ways and a variety of angles.
Avoid long periods of time in the car seat, swings, crib, floor. If you’re busy try baby wearing, this helps baby strengthening their neck as well as provides input in different ways to baby’s vestibular system.
Alternate head positions when baby is on their back to sleep.
Encourage baby looking in different directions by changing the direction they lay in the crib in relation to the door or hanging decorations.
Alternate sides of feeding
Alternate the positions and sides that baby is held on.
While the above activities help reduce the risk of plagiocephaly and torticollis, they also assist baby in the development of strong neck muscles and head control. This then has a carry over to a solid foundation to development of other gross motor skills.
How is Plagiocephaly/Torticollis Treated?
Your paediatrician will help monitor baby to ensure there are not other reasons contributing to the development of these things. They may want to rule out and monitor baby’s hearing and vision. Your paediatric dentist or lactation consultant may want to rule out tongue tie or lip tie as a contributing factor.
While the above is being monitored, a physiotherapist that treats paediatric patients can help treat and prevent these issues from worsening. The physiotherapist can assist with stretching, strengthening exercise as positioning while in clinic. They will also give parents activities for home.
If baby’s head shape is a concern or not resolving your paediatrician of paediatric physio may suggest a helmet from a specialized orthotist. A baby’s head will mould until 1 year of age. It is more helpful when baby is younger.
New parents can have a lot on their plate. These issues may seem overwhelming. Your paediatrician and physiotherapists will do their best to educate you and put your mind at ease. Small bits throughout the day is helpful.